

Grappling ranks amongst some of the most intense forms of exercise that an athlete can put their body through. Wrenching, pushing, pulling, submitting, throwing, and landing, usually against full resistance, all take their toll on the body, and the shoulder joint is a common site for musculoskeletal issues to arise. The reason why the shoulder joint is particularly susceptible to injuries lay in its very unique anatomy.
Unlike the hip joint which is a deep “ball and socket” joint, the shoulder joint (glenohumeral joint) is a much shallower joint that sits in a flatter socket (glenoid). This makes the shoulder much more mobile and versatile than the hip joint, but with that comes a sacrifice of stability.
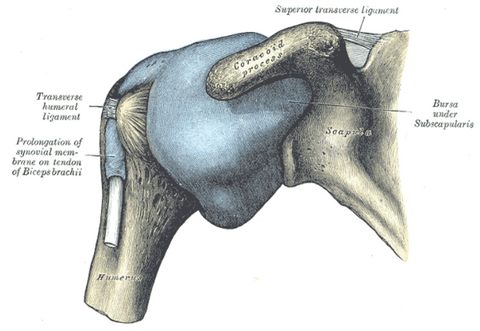
To aide stability of the joint, several structures are utilized, the main elements being the glenoid labrum which is a cartilaginous ridge that deepens the joint socket and the ligaments that cross directly over the joint. Further stability is achieved by a key group of muscles called the rotator cuff, which surrounds the joint and exerts a variety of influences to maintain the integrity of the joint while also being involved in all shoulder movements.
Mobility is further enhanced by the movement of the shoulder blade (scapula) on the rib cage (thorax) (scapulothoracic), the joint between the sternum and the collarbone (sternoclavicular), as does the joint between the collarbone (clavicle) and the tip of the shoulder blade which is called the acromion (acromioclavicular).
The combination of “glenohumeral” “acromioclavicular” “scapulothoracic” and “sternoclavicular” motion enables an almost endless scope of activity to be undertaken by the upper limb, so it is essential for any grappling athlete to take good care of their shoulder if they want to be enjoying this sport for the long term.

The posterior musculature of the shoulder joint
In this article, we will be exploring 7 of the most common clinical shoulder conditions for those involved in the grappling arts, namely Brazilian Jiu Jitsu and Submission Wrestling.
1: Rotator Cuff Tears:
Complete or partial tears in the rotator cuff musculature are extremely common in those involved in contact sports, particularly grappling arts. These tears are either partial or complete and usually occurs at the junction of where the muscle becomes tendon, termed the musculotendinous junction.
Patients presenting with these tears will often struggle to sleep on the affected side and their ability to perform overhead movements are often compromised. Diagnosis of tears is confirmed by MRI and although partial tears can respond well to manual therapy, complete tears will often require surgical correction, especially in younger athletes.
2: Rotator Cuff Tendinopathy:
These are usually overuse injuries, which irritate the rotator cuff tendon and are classified as Tendonitis or Tendinosis.
Tendonitis refers to a shorter duration (acute) tendon injury, accompanied by inflammation, which is characterised by pain, swelling, redness, heat, and loss of function. Tendinosis, on the other hand, is a longer-term (chronic) tendon issue with some degenerative changes, but without the inflammation seen in more acute cases. Such patients suffer from painful overhead activities, often night pain and may even have a history of instability/recurrent dislocations.
Treatment approaches to tendinopathies are wide and varied, from various forms of physical therapy, corticosteroid injection, all the way to ultrasound.
3: Impingement Syndrome:
This usually starts as a tendinopathy in a part of the rotator cuff called the supraspinatus, which causes a cascade of events, including increased nerve density in the affected tendon, the pain of which causes secondary muscle dysfunction, causing altered mechanics which lead to subacromial bursitis.
Other causes such as boney spurs from degenerative acromioclavicular or glenohumeral joints may also cause impingement. Similarly, and possibly coexisting with other conditions of the shoulder, the athlete will present with slow onset shoulder pain on lateral and overhead movements, weak shoulder movements, and difficulty laying on the affected side. However, the actual cause of the impingement needs to be accurately diagnosed and can be done by a clinical qualified practitioner, for treatment to be effective. Various treatment modalities are used to treat impingement syndrome, including anti-inflammatory drugs, manual therapy and exercise therapy.
4: Bursitis:
Bursae are lubricant filled sacks that sit around joints to reduce friction between adjacent structures and can become swollen and inflamed after traumatic events, or more commonly from overuse injuries. In grapplers, this usually occurs after impact on the shoulder joint itself or attempting to escape a vulnerable position against an opponents resistance.
Inflammation of the bursa is termed bursitis and although the shoulder joint has several bursae, it is the subacromial bursa that is usually affected by this condition and often presents alongside other shoulder problems such as impingement and/or tendonitis. If it remains unchecked for a long period of time, it can result in severe restriction of movements of the shoulder joint, often termed frozen shoulder.
The good news is that shoulder bursitis is quite responsive to an effective combination of pharmaceuticals, and manual alongside exercise therapy if rested adequately.
5: Acromioclavicular (AC) joint conditions:
This another common site for injury and shoulder pain, as it is anatomically vulnerable due to a lack of muscular support directly over the joint. Injury usually occurs after landing on the tip of the shoulder causing damage to the surrounding ligaments, often classified as one of the 6 types of AC joint injuries.
Surgical correction may be indicated in higher grade damage that has resulted in dislocations, whereas lower grade injuries can be treated similarly to other ligamentous injuries with anti-inflammatory drugs, rest, and physical therapy including the strengthening of the nearby musculature, namely the rotator cuff.

The acromioclavicular joint and surrounding ligaments
6: Labral Tears:
The labrum is a cartilage structure that sits on the rim of the socket of the shoulder joint and serves to increase the stability of the joint by increasing its depth, aiding muscular control, and spreading the load to the joint equally. Various mechanical stresses can damage the labrum, forced traction through the bicep such as when an opponent drives their leg to the ground defending the single-leg takedown.
A “cocked” throwing movement similar to what might be seen in an Americana may also damage the labrum, especially with explosive resistance. This shoulder pain may also be accompanied by clicking or popping as the loose labrum gets caught up between the joint surfaces. Only the mildest cases of labral damage can be treated without surgical intervention, and a full assessment and care from an experienced surgeon are recommended for those seeking a complete recovery, but manual treatments may be helpful in reducing local pain and inflammation prior or after more invasive procedures.
7: Dislocations:
These are amongst the most common traumatic shoulder injuries for grapplers, usually, the head of the upper arm moves forward relative to its socket similar to what you may see in a kimura that goes beyond the end of range. These may coexist with a fracture to part of the upper arm or shoulder blade and will often result in recurrent dislocations as the stability of the joint becomes compromised over the long term.
Dislocations require immediate medical care and relocation should only be carried out by qualified professionals, however, once back in place more conservative treatment approaches could help in reducing pain and inflammation and exercise programs can help reduce the risk of chronic instability of the joint occurring.
The above is by no means a complete list of injuries to the shoulder girdle that may occur in the grappling realm, but are the most common in my clinical experience.
















0 comments